Aging pagers and unreliable SMS: limited basement signal, no delivery confirmation. The doctor never knows if the message got through, the operator does not know whether to chase again.
Hospitals and CISSS networks
Reaching a doctor shouldn't depend on a pager or a text message
Critical messaging as simple as a pager, but made much better. The switchboard reaches the doctor with one click from IPA. The alert arrives on their smartphone with a dedicated ringtone, never confused with social media or email. They read, confirm and call back the extension. No pager, no anxiety telling notifications apart.
Sector challenges
Our answer
Guaranteed delivery, multi-channel
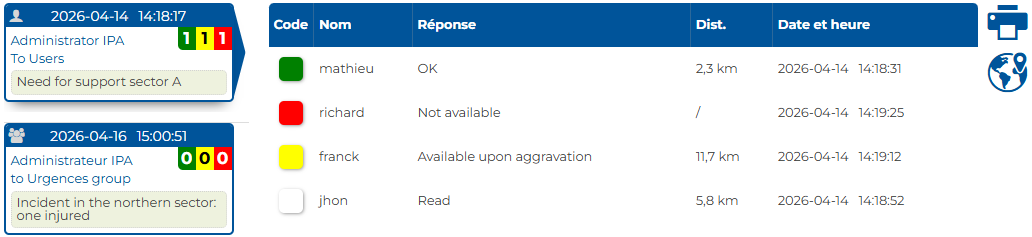
Simultaneous delivery through the mobile app, SMS and voice call. If one channel fails (no Wi-Fi, phone off, basement), the others take over. Received / Read / Answered status fed back to the operator in real time, for every alert.
Notifications lost in the noise: doctors cannot tell a hospital alert apart from a social media notification, an email or a personal text. The result: constant anxiety or alerts missed at night.
For the doctor: a sound they recognize
Important message displayed directly on the lock or standby screen, with dedicated ringtone and strong vibration. Overrides silent mode AND Do Not Disturb (DND). Never confused with social media, email or a personal text. The doctor reads, confirms with one tap and sees the extension to call back.
Blind switchboard, no unified tool: multiple software, paper, emails to track in parallel. No way to know whether the alert was received or when the doctor will call back.
For the operator: everything on one page
A single web console: Received / Read / Answered status of every message in real time, quick new-message sending, shared notes between operators and notes on doctors (availability, preferences, contacts). No extra window, no additional app to learn.
Complex on-call schedules: multiple calendars on paper or spreadsheet, last-minute substitutions, internal groups (Code Blue) and external-facing groups (psychosocial, domestic violence) managed separately. Every mistake costs clinical time.
Flexible groups, with or without dedicated line
Each group can have its own dedicated phone line when external access is useful (psychosocial, domestic violence, specialty open to 811) or stay purely internal with no number (Code Blue, quality team). Shared on-call schedules, one-click substitutions.
Hidden costs and false compromises: a pager fleet is expensive to manage (rental, batteries, replacements, losses), and SMS look free but offer no critical delivery guarantee. The real cost of alternatives is usually higher than it appears.
Pricing adapted to your scale
Two models depending on your scale. Large CISSS networks: usage-based model, $4.50 per active user in the month — pay only for people actually contacted. Hospitals and smaller establishments: per-enrolled-user pricing, volume- and term-tiered. No hardware, no pager to replace.
In practice: from call to callback, 60 seconds
A nurse calls the switchboard: she needs the on-call cardiologist for an urgent consultation on a patient at extension 5423. The operator opens IPA, picks the « Cardiology on-call » group and sends: Patient at extension 5423, urgent, cardio.
Within 2 seconds, the on-call cardiologist receives the alert on their smartphone with strong vibration and the dedicated IPA ringtone. They confirm with one tap, the operator sees the confirmation in real time, and the cardiologist calls back extension 5423. No pager, no manual callback, everything logged.
1,200 pagers
replaced in 6 weeks at a single CISSS, with no service interruption
Already deployed at CISSS de Lanaudière, CISSS des Laurentides, CIUSSS du Saguenay–Lac-Saint-Jean, CISSS de Chaudière-Appalaches, CISSS de la Côte-Nord, CISSS de l'Outaouais — and others.
CISSS implementation program
IPA features activated in this sector
Frequently asked questions
Does IPA replace our phone system?
No. IPA does not replace your switchboard or your telephony. We are complementary: your switchboard keeps receiving calls, and the operator uses IPA as a new alerting tool toward doctors in place of the pagers.
How does the operator send a message?
Through the IPA web console: a single page for everything. The operator sees Received / Read / Answered status in real time for each message, sends a new message by picking the recipient (individual doctor or group), can use templates (callback extension, Code Blue, etc.) and consult notes shared by the team. Typical training: 15 minutes.
How long does rollout take?
We supported a CISSS in replacing 1,200 pagers in 6 weeks. For a single hospital, count 2 to 4 weeks. We handle group configuration, staff directory import, and training.
Can we keep pagers during the transition?
Yes. IPA can send in parallel to legacy pagers (via SNPP) and to smartphones. Doctors switch gradually, with no service interruption or panic.
How does the doctor tell an IPA alert apart from a personal notification?
The IPA app has its own dedicated ringtone, recognizable from the first second and distinct from other notifications (social media, emails, personal texts). The message appears directly on the lock or standby screen, readable without unlocking. IPA overrides silent mode AND Do Not Disturb for critical alerts. No more anxiety at every ambient beep, and zero missed alerts at night.
How are teams reached when called by 811 or by external services outside the hospital?
Each team or specialty can have its own dedicated phone line when external access is desired. An incoming call from 811, an external call center, another facility or a lab is routed instantly through IPA to the on-call person in the group, based on the schedule. Internal groups that do not need external access (Code Blue, quality team) work without a dedicated line. 24/7 access.
How does pricing work?
Two models depending on your size. Large CISSS networks: usage-based, $4.50 per active user in the month (pay only for people actually contacted). Hospitals, smaller CIUSSS, clinics: per-enrolled-user pricing, from $4 / user / month. In either case: no hardware, no per-pager contract, no pager to replace.
365 × 24/7 support — infrastructure in Quebec
The solidity a critical infrastructure demands.
24/7 human support
Our team is reachable at all times. No bot, no lost ticket — engineers who know your deployment.
Hosting in Quebec
Servers located in Quebec, compliant with Quebec's Bill 25. Your data stays on Canadian soil.
Redundant infrastructure
Redundant servers, encrypted backups, 24/7 monitoring. Availability is our foremost commitment.
Try IPA in your hospital — no commitment
Full account created in minutes. A dedicated team at your disposal for unlimited testing. Multiple CISSS networks have already adopted it — your turn?